Greetings
Thank you to all who came out to help make Dr. David Sahley's Balance Seminar a success last week. We will let you know the next time we have a seminar available in the area. If you have any questions regarding last weeks topic of fall prevention, please feel free to give us a call anytime and we would be happy to help. Thank you again.
This edition of our newsletter is focussed on shoulder pain from rotator cuff tears.
If you’re over the age of 30, and you’re experiencing pain and weakness in your shoulder, you’re probably suffering from a rotator cuff disorder. Simple everyday activities like changing your clothes or bathing can be made uncomfortable or even impossible. These significant, but often understated conditions involve irritation of the tendons and muscles that help connect the upper arm bone w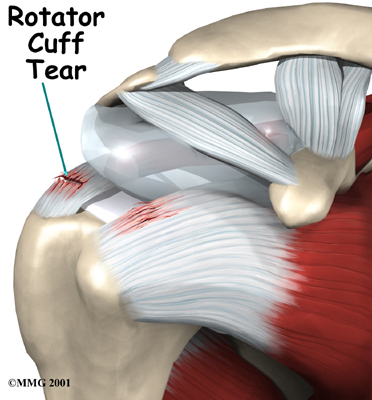 ith the shoulder blade. ith the shoulder blade.
Historically, these conditions were thought to primarily involve tendinitis, or inflammation of the tendons, and bursitis, or inflammation of the fluid-filled sacs between tendons and the shoulder blade. More recently, comprehensive clinical examinations have shown that conditions related to the overuse of tendons are more consistent with muscle tissue degeneration, and often occur in the absence of inflammation. Also referred to as tendinosis, the causes of tendon or muscle tissue degeneration are often unknown.
Although rotator cuff issues are often caused by the types of repetitive overhead motions used during sports like badminton, tennis and racquetball, they can also be caused by repetitive work-related stress and strain. Rotator cuff disorders can also be caused by poor posture, acute injury due to falling, or simply due to the everyday muscle and tendon degeneration that accompanies the normal aging process, and wear and tear.
In addition to tendinitis, bursitis and tendinosis, sudden rotator cuff tears after a fall or injury may occur and are associated with debilitating pain and often surgical treatment of the affected rotator cuff. Unfortunately, the success of surgery is dependent on a variety of factors, and incomplete recovery and a worsening of rotator cuff syndrome pain has been reported to be as high as 23% to 35% of the time.
Fortunately, physical therapy for rotator cuff disorders can significantly improve the range of motion and pain management of the affected rotator cuff, especially after surgical treatment. Depending on the underlying causes and extent of the rotator cuff issue, the following treatment options may be recommended to help improve function and relieve pain:
1. Stretching Exercises.
A variety of range of motion exercises are used to help exercise muscle groups of the rotator cuff to help promote joint flexibility and to reduce the risks of joint mobility issues. Stretching exercises include pendulum stretches, which help stretch the area where tendons move; posterior capsule stretches, whim aim to ease the tightness of the ligaments near the back of the shoulder and help to eliminate rotator cuff pain; and wand exercises, which involves improving the range of motion of the shoulder joint.
2. Strengthening Exercises.
Strengthening muscles of the rotator cuff helps to prevent re-injury. These exercises include scapular squeezes and setting, inward and outward rotation exercises, and abduction exercises.
By combining stretching and strengthening exercises into a personalized regimen, physical therapists are capable of significantly reducing the recovery time following surgery and greatly increase muscle strength and the range of motion of the affected rotator cuff. Although a variety of exercises will be recommended for patients to complete at home, studies have shown that the specialized supervision of a trained physical therapist allows for a significantly better recovery after rotator cuff surgery.
For more information on how physical therapy can effectively help those with rotator cuff disorders, please contact the trained and licensed physical therapists at Dynamics Physical Therapy. We would be pleased to examine your shoulder, and develop a personalized physical therapeutic treatment plan that specifically addresses your needs.
Read more on rotator cuff tears here.
References
- Silverstein B, Welp E, Nelson N, Kalat J. Claims incidence of work-related disorders of the upper extremities: Washington state, 1987 through 1995. Am J Public Health. Dec 1998;88(12):1827-1833.
- Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome. A critical review. Clin Orthop Relat Res. Aug 1991(269):162-173.
- Tytherleigh-Strong G, Hirahara A, Miniaci A. Rotator cuff disease. Curr Opin Rheumatol. Mar 2001;13(2):135-145.
- Childress MA, Beutler A. Management of chronic tendon injuries. Am Fam Physician. Apr 1 2013;87(7):486-490.
- Wilson JJ, Best TM. Common overuse tendon problems: A review and recommendations for treatment. Am Fam Physician. Sep 1 2005;72(5):811-818.
- Razmjou H, Lincoln S, Axelrod T, Holtby R. Factors contributing to failure of rotator cuff surgery in persons with work-related injuries. Physiother Can. Spring 2008;60(2):125-133.
- Abate M, Schiavone C, Di Carlo L, Salini V. Prevalence of and risk factors for asymptomatic rotator cuff tears in postmenopausal women. Menopause. Jun 10 2013.
- Huberty DP, Schoolfield JD, Brady PC, Vadala AP, Arrigoni P, Burkhart SS. Incidence and treatment of postoperative stiffness following arthroscopic rotator cuff repair. Arthroscopy. Aug 2009;25(8):880-890.
- Kartus J, Kartus C, Rostgard-Christensen L, Sernert N, Read J, Perko M. Long-term clinical and ultrasound evaluation after arthroscopic acromioplasty in patients with partial rotator cuff tears. Arthroscopy. Jan 2006;22(1):44-49.
- Odenbring S, Wagner P, Atroshi I. Long-term outcomes of arthroscopic acromioplasty for chronic shoulder impingement syndrome: a prospective cohort study with a minimum of 12 years' follow-up. Arthroscopy. Oct 2008;24(10):1092-1098.
- Ogilvie-Harris DJ, Wiley AM, Sattarian J. Failed acromioplasty for impingement syndrome. J Bone Joint Surg Br. Nov 1990;72(6):1070-1072.
- Escamilla RF, Yamashiro K, Paulos L, Andrews JR. Shoulder muscle activity and function in common shoulder rehabilitation exercises. Sports Med. 2009;39(8):663-685.
- Kachewar SG, Kulkarni DS. Calcific tendinitis of the rotator cuff: a review. J Clin Diagn Res. Jul 2013;7(7):1482-1485.
- Long JL, Ruberte Thiele RA, Skendzel JG, et al. Activation of the shoulder musculature during pendulum exercises and light activities. J Orthop Sports Phys Ther. Apr 2010;40(4):230-237.
- Strickland JP, Fleckenstein CM, Ducker A, Hasan SS. Early Results of Concurrent Arthroscopic Repair of Rotator Cuff and Type II Superior Labral Anterior Posterior Tears. Sports Health. Nov 2010;2(6):503-508.
- Litchfield R. Progressive strengthening exercises for subacromial impingement syndrome. Clin J Sport Med. 2013;23(1):86-87.
- Holmgren T, Oberg B, Sjoberg I, Johansson K. Supervised strengthening exercises versus home-based movement exercises after arthroscopic acromioplasty: a randomized clinical trial. J Rehabil Med. 2012;44(1):12-18.
|
|